
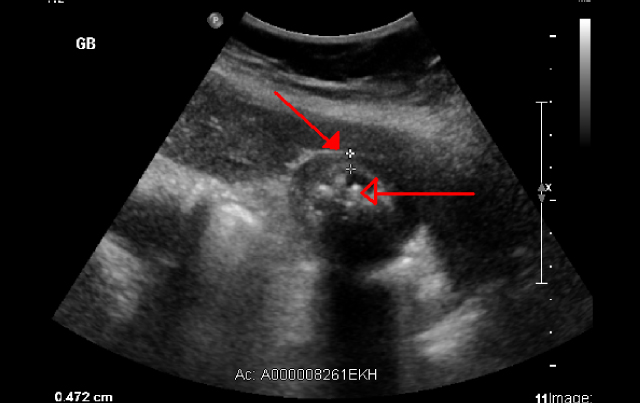
Diagnosing Acute Cholecystitis

Christopher May, MD
With improvements in ultrasound technology over the past two decades, some have questioned the need for hepatobiliary iminodiacetic acid (HIDA) scans for diagnosing acute cholecystitis. However, this underutilized modality, especially when sonographic findings are equivocal or negative, still has considerable value.
In a meta-analysis of 57 diagnostic trials in 5,859 adult patients, researchers evaluated diagnostic accuracy of HIDA, ultrasound and MRI. They found that the sensitivity for HIDA at 96 percent was significantly higher than either MRI (85 percent) or ultrasound (81 percent). Perhaps more important for clinicians, when HIDA was performed after a negative ultrasound, there was a statistically significant increase in sensitivity from 40 percent to 85 percent. There was no such improvement for ultrasound performed after negative HIDA.
This is a typical situation for patients thought to have acute cholecystitis, says Chris May, MD, a nuclear medicine radiologist at Scottsdale Medical Imaging (SMIL). While the sensitivity for ultrasound has improved to the range of 60 to 80 percent in most studies, he says, the sensitivity and negative predictive value for HIDA is still considerably better than ultrasound.
“If you think someone might have acute cholecystitis and you do a HIDA scan and it is normal, the chances of the patient actually having acute cholecystitis are minuscule, less than 1 percent in some studies,” May says. “It is very helpful for ruling it out. I still think the hepatobiliary scan is the single most accurate method of looking at cholecystitis.”
Researchers at Rutgers-Robert Wood Johnson Medical School conducting a smaller 2013 retrospective review of 154 patients reached a similar conclusion. They found that ultrasound has the potential of rendering other tests unnecessary when sonographic features of cholecystitis are present. They concluded, however, that a HIDA scan is superior to ultrasound in diagnosing cholecystitis, having higher sensitivity, specificity and accuracy than ultrasound.
May adds that in the opposite case the hepatobiliary scan is also superior to ultrasound. “If you do an ultrasound on a patient and it shows no evidence of cholecystitis but the symptoms indicate otherwise, at that point the HIDA really does have some added value,” May says. “And it can also be especially helpful for the atypical presentations seen in older people and diabetics. You don’t want to miss an acute cholecystitis in anyone, but particularly so if the patient is diabetic.”
REFERENCES:
Chu M, Coulter L, Hudson J. Which imaging modality is the best to diagnose acute cholecystitis?
Evidence-Based Practice. 2014;17(5):E2.
Bernescu I, Eng O, Potdevin L, et al. Is HIDA scan necessary for sonographically suspicious
cholecystitis? J Curr Surg. 2013;3(2):62-65.
