
Adhesive capsulitis (AC) or “Frozen Shoulder”

Jeffrey Fitzergald, MD
Adhesive capsulitis (AC), or “Frozen Shoulder,” is a relatively common female predominant condition found in 3% of the general population. Clinically it is defined by progressive pain/decreased range of motion (ROM) corresponding to synovial inflammation and capsular fibrosis pathologically. Once thought solely as a clinical diagnosis, there are now readily identifiable MR imaging features that are highly suggestive and in some cases diagnostic of adhesive capsulitis in the proper clinical setting.
Frozen shoulder can be idiopathic or secondary, with known associations to trauma, prior surgery, diabetes, and hypothyroidism. It is classified into 4 clinical stages ranging from limited ROM/pain (stage 1), “freezing” stage characterized by severely restricted ROM/pain (stage 2, most common stage at presentation), “frozen” stage (stage 3), and “thawing” stage (stage 4) characterized by improving ROM/minimal pain. AC can mimic and in some cases coexist with other more serious conditions such as rotator cuff tear, labral tear, and osteoarthrosis. MRI plays a critical role in distinguishing between these processes.1
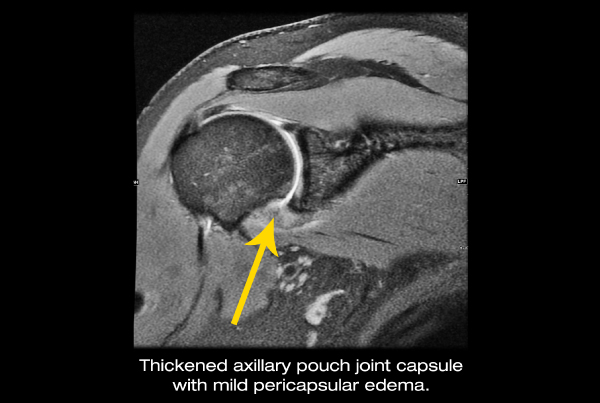
Classic imaging features of adhesive capsulitis include thickening and high T2 signal within the axillary pouch joint capsule/inferior glenohumeral ligaments, thickening of the coracohumeral ligament, and scar tissue formation within the subcoracoid as well as
rotator interval fat. While one or any combination of these findings can be suggestive of the condition, capsular high T2 signal has the highest sensitivity and specificity approaching 88%.2
In general the condition is self-limiting however it can take 18-30 months for symptoms to resolve. Prompt identification on MR is crucial in guiding proper management. If symptoms are attributable to adhesive capsulitis, intra-articular steroid injection along with physical therapy have been proven to shorten duration of symptoms, significantly reduce patient morbiditiy, and improve function. This minimally-invasive procedure can be done with fluoroscopic or ultrasound guidance to ensure intra-articular administration of the medication. SMIL performs many of these a day. In rare cases unresponsive to this, arthroscopic capsulotomy and shoulder manipulation under general anesthesia to break up capsular scar tissue have been proven effective treatments.
REFERENCE:
1 Mengiardi, et al; “Frozen Shoulder: MR Arthrographic Findings,” Radiology 2004; 233:486 – 492
2 Teixeira et al, “Adhesive capsulitis of the shoulder: Value of inferior glenhumeral ligament signal changes on T2-wighted fat-saturated images.” American Journal of Roentgenology. 2012;198: W589-W596.
